




Are you interested in exploring what your life might be like with a healthier, higher-performing brain and body? We are!
Click below to schedule a free consultation!!
Imagine taking your seat in a crowded theater to watch the debut of a highly anticipated show. The lights dim, silence ensues, the curtain rises. All of a sudden bout of hiccups begins. Each 'hic' that comes out of your mouth causes awkward looks and after a dozen, begins to elicit frustration from the crowd. This is a scenario many of us can relate to. I've been there too. But through a combination of understanding the body's mechanisms, applying principles of functional neurology, and leveraging certain physiological reflexes, I've developed a method to stop hiccups in their tracks—usually in less than 20 seconds, and it works nearly every time. Best yet, it doesn’t require drinking, standing on your head, getting scared, or any of these other random, ineffective methods.
Hiccups are a common and curious medical phenomenon characterized by involuntary, repetitive contractions of the diaphragm—the primary muscle involved in breathing. These spasms result in a distinctive and (sometimes) humorous ‘hic’ sound, which occurs due to the abrupt closure of the glottis following a swift intake of air. Medically known as “singultus,” the term hints at the nature of hiccups, translating from Latin to mean “the act of catching one’s breath while sobbing.” While hiccups are a nearly universal experience, often appearing without warning, they remain a surprisingly mysterious function of the human body.
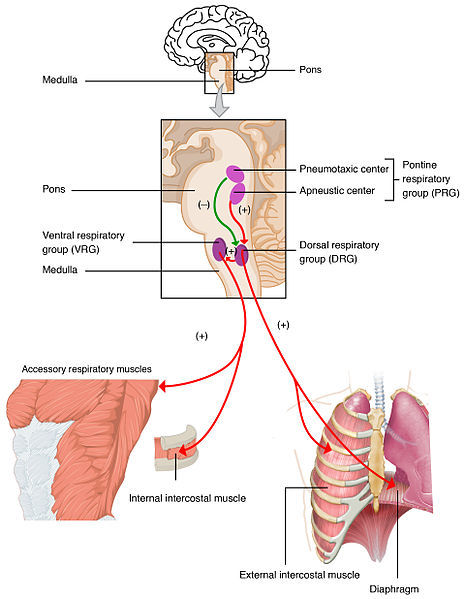
The physiological process of hiccupping involves a complex reflex arc that starts with an involuntary contraction of the diaphragm and, occasionally, the intercostal muscles which lie between the ribs. Following the contraction, air is quickly sucked into the lungs, and almost instantaneously, the glottis (the part of the larynx consisting of the vocal cords and the slit-like opening between them) closes sharply. This closure quickly and abruptly stops the inflow of air and produces the characteristic ‘hic’ sound of the hiccup. This sequence is controlled by a reflex arc that includes afferent nerves like the phrenic and vagus nerves, central neurological pathways in the brain stem, and efferent nerves that signal the muscles to contract.
Immediate onset, short duration bouts of hiccups are inconvenient and often frustrating, but ultimately are self-resolving. These types of hiccups can be triggered by numerous factors that may disrupt normal diaphragm function. Commonly, they are caused by simple physical stimuli such as eating too quickly, consuming overly hot or spicy foods, or ingesting alcohol and carbonated beverages, leading to stomach distension. However, hiccups can also be induced by conditions affecting the gastrointestinal or central nervous systems, such as reflux or even Parkinson’s disease. Emotional triggers like stress, excitement, or anxiety are also known to provoke hiccups, particularly through mechanisms like over-breathing or swallowing air, a condition known as aerophagia.
In some cases, hiccups may persist for an extended period, which could indicate underlying medical issues and warrant further investigation. Medical consultation is recommended for persistent or severe hiccups that last more than 48 hours as they could be a symptom of a more serious condition. However, hiccups generally occur due to a functional dysregulation of the pace of inspiration and expiration, almost like a twitch or myoclonic jerk.
Here is a comprehensive list of conditions that may cause hiccups (PMID: 26307025): Abdominal abscess, Abdominal tumours, Alcohol, Anaesthetic agents, Anxiety, Antibiotics (e.g. macrolides), Asthma, Barbiturate, Benzodiazepines, Bowel obstruction, Brain injury, Bronchial carcinoma, Bronchitis, Chemotherapy (platinum-based agents), Diabetes mellitus, Dopamine agonists, Endoscopy, Encephalitis, Epilepsy, Excitement, Fear, Foreign body in nose or ear, Gastro-oesophageal reflux disease, Herpes zoster, Hiatus hernia, Hypocalcemia, Hypocapnia, Hypokalemia, Hyponatremia, Intracranial tumour, Ischaemic/haemorrhagic cerebrovascular insult, Meningitis, Multiple Sclerosis, Myocardial ischaemia, Neuromyelitis optica, Oesophagus cancer, Opioids, Otitis, Pancreatitis, Parkinson's Syndrome, Peptic ulceration, Pericarditis, Peripheral nervous system (phrenic, vagal and sympathetic nerves), Pharyngeal intubation, Pharyngitis, Placement of central venous catheter, Pneumonia, Psychosomatic disorders, Renal impairment, Rhinitis, Steroids, Stomach distension, Stress, Surgical injuries, Thoracic aneurysm, Thoracic and upper abdominal surgical, Toxic metabolic, and Tuberculosis.
When no particular pathology is determined or if a definitive cure is unattainable, various physical and pharmacological treatments are available for managing hiccups. Generally speaking, maneuvers that have been suggested are effective at shortening an attack of acute hiccups but not the treatment of persistent or intractable hiccups. None have been subjected to clinical trials, and you can probably attest to the lack of efficacy of many.
These remedies are mainly anecdotal and range in effectiveness from barely effective, to a total waste of time.
An (equally lengthy) list of drugs is suggested for curing hiccups, underscoring the incomplete understanding of the underlying pathophysiology and the fact that no single treatment proves effective for most cases.
As long as you are not on one of the 78 drugs that interact with it, the first drug prescribed for hiccups is a treatment trial of proton pump inhibitors (PPIs) with alginate reflux suppressants like omeprazole (Prilosec).
If a person does not respond to Prilosec, then empirical therapy is as follows:
First Line:
Second Line:
Third Line:
Other Choices:
Concerns Associated with These Medications:
The medications listed vary in their side effects, which are crucial to consider when prescribing. Common issues include sedation, which can affect daily activities and safety, especially in drugs like Baclofen, Gabapentin, and Chlorpromazine. Neurological side effects are also a significant concern with many of these medications, including clumsiness, mood disturbances, and more severe outcomes like neurological impairment seen with Metoclopramide and Domperidone. Cardiac issues such as arrhythmias can occur with drugs like Domperidone and Amitriptyline, especially at high doses or in overdose situations. Other serious concerns include renal impairment with Baclofen in older patients, respiratory difficulties with Pregabalin, liver failure with Valproate, and hypotension with Nifedipine. These side effects necessitate careful patient monitoring and consideration of individual patient risk factors when prescribing these medications.
Many of the so-called "tricks" for stopping hiccups amount to little more than comical antics. From someone startling you, to sipping water, drinking water while upside down, or merely holding your breath, these methods lack any substantial scientific rationale or support. The medications used for persistent or intracticble hiccups have (sometimes serious) side effects. However, if we look a bit deeper, they all share a common theme: they all aim to alleviate the condition by acting on relevant neurological pathways.
So I began to think…
If an uncontrolled inspiration reflex causes hiccups, maybe (like many other reflexes) there’s another reflex that counteracts and suppresses that reflex. That’s when I had a flashback to a reflex that was taught in our first semester of neurophysiology in Chiropractic school by Dr. Rigby; the Hering Bruer reflex
The Hering-Breuer Inspiratory Reflex, first identified in 1868 by Ewald Hering and Joseph Breuer, is the earliest studied pulmonary reflex and is named after its discoverers. This reflex has been extensively examined in both physiology and pathology and shows remarkable consistency across different mammalian species.
The reflex serves as a neurological mechanism that prevents lung overinflation. While breathing is essential for survival, excessive inhalation can be detrimental. The Hering-Breuer reflex not only prevents hyperinflation in adults but also helps establish and regulate rhythmic breathing patterns in infants.
The underlying neurologic process of the Hering-Breuer reflex is a sophisticated example of an inhibitory feedback loop. It starts with the activation of high-threshold mechanoreceptors in the lungs, which are sensitive to intense mechanical stretching. When the lungs inflate beyond their usual capacity, these receptors begin to send signals via the vagus nerve (Cranial Nerve 10) to a specific area in the nucleus tractus solitarius (NTS). In the NTS, specialized neurons known as "pump cells" receive these signals. These pump cells then relay information to brain regions that neurologically suppress further inhalation, effectively preventing over-breathing or reflexive actions like hiccups.
How can you expand your lungs sufficiently to activate pulmonary stretch receptors and pump cells?
With aging, the threshold required to trigger the Hering-Breuer Reflex (HBR) increases. It's believed that for adults, the intensity needed to stimulate the HBR grows exponentially, starting at about 1 liter beyond the typical breathing volume (2-3 liters), and can reach up to a maximum capacity of around 6 liters. Therefore, theoretically, to activate the HBR, one must inhale enough air for the brain to perceive that any additional intake could be harmful.
Disclaimer: The information provided herein is for informational purposes only and is not intended as medical advice, diagnosis, or treatment. You should consult your physician or healthcare provider before using this information to diagnose or treat any health problems or illnesses, including hiccups. The author assumes no liability for any injury, loss, or damage caused or alleged to be caused directly or indirectly by any treatment, action, or application of any method discussed in this material. If you have any concerns about your health, you should always consult with your physician or a healthcare professional familiar with your health. Use of the information and techniques described is at the sole discretion and risk of the user.
As soon as I have that second hiccup, I follow this procedure:
Step 1: Inhale as deeply as possible
Step 2: Plug my nose and close my mouth
Step 3: “Sip” more air in through my lips without letting air out, as if I were sipping on a straw.
Step 4: Repeat Step 3 until I cannot fit any more air in my lungs (typically 3-10 sips)
Step 5: Hold that air in my lungs for 10 seconds
Step 6: Breathe out and breathe naturally
At this point, 100% of the time that I’ve done this for myself or had someone do it, their hiccups are gone!
Functional neurology harnesses a deep understanding of the intricate interactions between the brain and body to develop unique, science-based interventions for various conditions, including seemingly minor yet persistent issues like hiccups. This discipline explores the specific neurological pathways involved in the onset of hiccups, crafting targeted therapies that can effectively reset these neural circuits. By focusing on the neurophysiological bases of symptoms rather than just the symptoms themselves, functional neurology offers a sophisticated approach to treatment that goes beyond traditional methods. These interventions are particularly valuable for conditions where conventional therapies may not provide relief or could introduce undesirable side effects. Functional neurology not only addresses the immediate problem, but also solves underlying dysfunction through innovative, tailored strategies that leverage the latest scientific insights into brain-body dynamics.
Do you have a problem that you wonder if functional neurology can solve? We want to hear from you!
